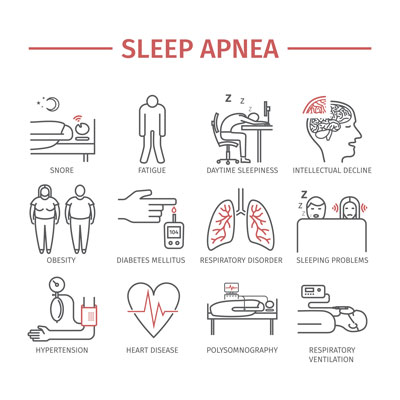
 Over the course of the last 20 years, my practice has continued to emphasize the importance of Sound Sleep as our #1. health priority. Nutrition close behind at #2. Exercise at #3. Poor quality sleep is the slow silent suicide that sucks the life-giving oxygen out of every function of the body especially the brain. How much nightly brain damage are you willing to accept for yourself and your loved ones? Sleep apnea, snoring, mouth breathing, grinding/clenching. TMJ problems, acid reflux, insomnia, and little blue lights from cell phones and iPad all conspire to damage your health with alarming consequences.
Over the course of the last 20 years, my practice has continued to emphasize the importance of Sound Sleep as our #1. health priority. Nutrition close behind at #2. Exercise at #3. Poor quality sleep is the slow silent suicide that sucks the life-giving oxygen out of every function of the body especially the brain. How much nightly brain damage are you willing to accept for yourself and your loved ones? Sleep apnea, snoring, mouth breathing, grinding/clenching. TMJ problems, acid reflux, insomnia, and little blue lights from cell phones and iPad all conspire to damage your health with alarming consequences.School performance, athletic performance, workplace performance, driving performance, mental health, and ability to cope with the stressors of life depend on the quantity and quality of sleep. We are just waking up to the fact that we are sleep deprived and have bought into the myth that to become a high achiever you need to cut back on slumber to accomplish more during the day. Quite the opposite is true, top performers sleep better than you do.
Sleep’s reparative and restorative functions depend on the duration or overall percent of total sleep time with Stage 3 (slow brain wave) and REM (rapid eye movement) being the most important, but only high-tech devices record these two parameters. Home sleep studies are an inexpensive limited test that gives helpful information for most situations but is not as accurate as an overnight sleep lab test.
Dysfunctional breathing is the root cause of most sleep disorders because airflow to the lungs is disrupted by inflammatory restrictions, anatomical restrictions, or neurological restrictions. Laminar (not turbulent) airflow must enter the nose (not mouth) and get to the lungs unimpeded. Sounds simple, but oh so complicated!
Two devices, CPAP (continuous positive air pressure) and MAD (mandibular advancing device) are effective at opening up the airway. CPAP the “gold standard” blows air down to the lungs while MAD mechanically moves the lower jaw forward to remove the soft palate/tongue obstruction thus increasing the size of the airway. Compliance with CPAP after one year is historically poor whereas oral devices are more comfortable and compatible. For some unknown unscientific reason, many sleep doctors do not recommend MADs because they take knowledge, skill, and time to adjust to the “sweet spot” and only experienced dentists have the know-how. Sleep docs know CPAP will work the first night it is worn whereas a MAD might take several weeks to properly adjust. The standard of success with either is the same.
Many patients are glad to have a MAD, they are comfortable, simple, and silent. My wife’s sleep has been improved remarkably much to the surprise of her cardiologist who never considered sleep apnea until I sent him results from our home sleep test. Then I had to convince him to let her try the MAD we had made, before his prescribing CPAP. Her sleep improvement is remarkable and she doesn’t have to hook up to an awkward machine every night.
Now you know why I am MAD glad. We can help you identify your sleep issues and get you on track to a healthier longer more enjoyable life of good sleep. SOS -save our sleep
John B. Harrison DDS, MSc
Orthodontist